How Texas Dental Practices & Medical Clinics Cut Electricity Costs 20–30% in 2026
Running a dental practice, urgent care clinic, or small medical office in Texas means managing sterilization equipment, vaccine refrigeration, HVAC systems, and patient-grade lighting—all drawing power simultaneously during peak afternoon hours when ERCOT rates climb. The result: most small practices pay 18–28% more per kWh than competitive market rates, simply because they’ve never run a real competitive bid or optimized their load patterns within existing operating hours.
This guide covers exactly where that money goes, what you can change without compromising sterilization schedules or patient care, and how to approach your contract strategically. Practices following this framework typically save $8,000–$28,000 annually depending on size, location, and starting rate.
Why Medical Practices Overpay—and Why It Persists
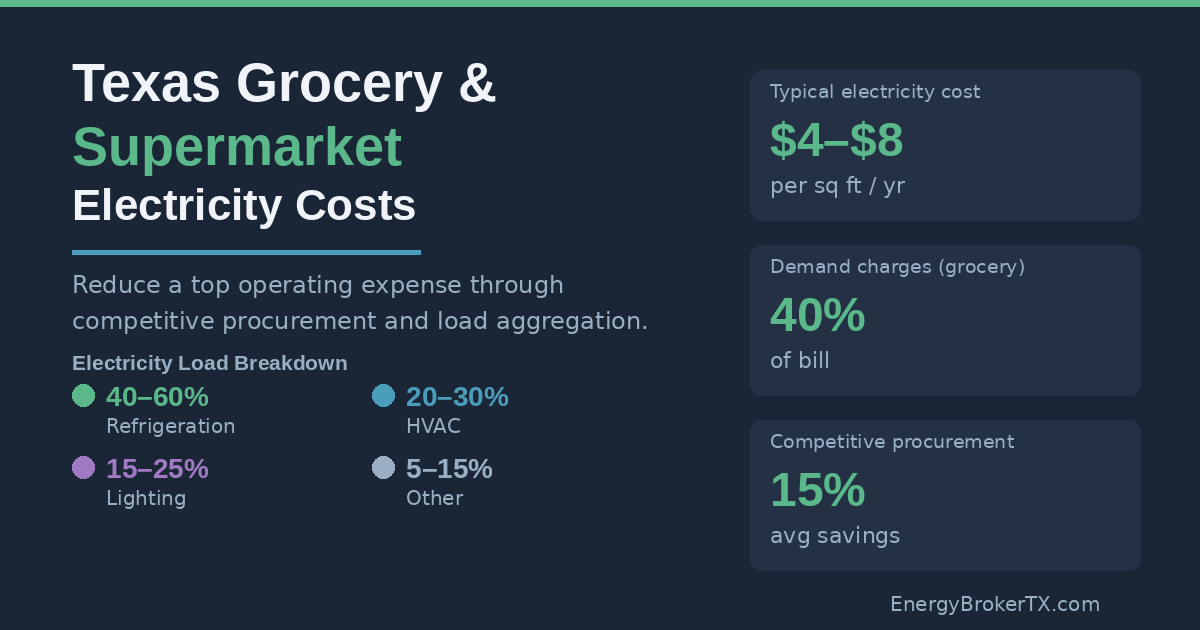
Small medical practices consume 8,000–30,000 kWh per month, with peak demand concentrated during the hours healthcare regulations require you to be fully operational. A typical autoclave draws 4–6 kW per sterilization cycle. Surgical overhead lights run 500–1,000W each. Ultrasound and imaging equipment, patient monitors, and the HVAC system handling infection-control air exchanges—all running simultaneously between 10 AM and 5 PM, exactly when ERCOT wholesale prices are highest.
That’s not a scheduling problem you can fully solve—patients arrive when they arrive. But it creates two compounding cost drivers that most practice owners don’t identify separately: the energy rate you’re paying per kWh, and the demand charge triggered by your peak 15-minute interval each month. Most practices focus on neither.
The second problem is procurement. The majority of dental practices and small clinics auto-renew with their existing provider and never see competitive pricing. Current market rates for medical practices in ERCOT-deregulated territories range from 7.8–9.2¢/kWh for competitively bid contracts. Practices currently paying 10.5–12¢/kWh are typically on auto-renewal pricing—a de facto penalty rate for inaction.
The math is direct: a 4-room dental practice in Dallas consuming 18,000 kWh/month at 11.5¢/kWh pays $2,070/month ($24,840/year). That same practice on a competitively bid rate of 8.2¢/kWh pays $1,476/month ($17,712/year)—a $7,128 annual reduction with zero changes to operations, staffing, or patient schedule.
Small practices have historically been underserved by brokers because their monthly volumes generate lower absolute commissions than large commercial accounts. Many dental and medical offices never receive a competitive bid at renewal. This is solvable—and the savings opportunity is real.
Decoding Your Medical Office Electricity Bill
Three components drive your bill. Each has different characteristics and different potential for reduction.
Energy charges represent 60–65% of a small practice’s total bill. This is the per-kWh rate set by your Retail Electric Provider (REP)—the number you’re actually competing when you solicit quotes. Current competitive rates for medical offices across Houston, Dallas, Fort Worth, and ERCOT-served markets: 7.8–9.5¢/kWh depending on term length and load profile. Everything in this category is negotiable.
Demand charges account for 25–35% of most medical office bills—and they’re the most frequently misunderstood. Even small practices typically have demand metering. Your peak 15-minute interval during the billing month determines your demand charge. A 45 kW peak during one afternoon translates to $50–$65 added to that month’s bill at current demand charge rates. If that peak occurs during a summer afternoon when ERCOT’s systemwide load is highest, it may also affect your transmission cost allocation for the following 12 months through the 4CP mechanism.
TDSP delivery charges are regulated utility pass-throughs running 10–15% of your bill. Identical across all providers in a territory—switching REPs doesn’t change them. As of September 2025: Oncor (Dallas/Fort Worth) runs approximately $4.23/month plus 5.60¢/kWh; CenterPoint (Houston) runs $4.90/month plus 5.90¢/kWh. These adjust each March and September. Understand them, but don’t spend time trying to negotiate them.
What’s Driving Costs Higher in 2026
ERCOT’s December 2024 capacity report projects 14% demand growth in 2026, driven primarily by data center and AI compute facility interconnection. That load growth tightens reserve margins and increases scarcity pricing events during summer peak hours—which flows into the risk premiums REPs embed in retail fixed-rate contracts.
ERCOT nodal wholesale prices averaged $35–40/MWh in 2024. Forward market curves point toward $48–55/MWh in 2026. At the utility level, Oncor and CenterPoint have filed rate increases in each of the past four TDSP adjustment cycles as post-Winter Storm Uri grid hardening costs work through rate recovery. These baseline delivery cost increases affect every medical practice equally.
For medical offices specifically: your fixed daytime hours (8 AM–6 PM) expose you to peak pricing by default. Unlike retail or manufacturing operations that can shift hours or production windows, medical practices have limited flexibility on when patient care happens. The opportunity is managing equipment loads within those hours—and that’s where the actionable savings live.
Competitive Procurement for Healthcare Accounts
A reverse auction process for a medical practice works differently than for large commercial accounts—and the outcomes are often better than practice owners expect. Smaller practices with predictable, stable load profiles are efficient for REPs to price. Medical offices have high location stickiness (patients are tied to a practice), which reduces supplier churn risk. Annual load variation is lower than seasonal businesses, reducing forecasting uncertainty. These factors make small healthcare accounts attractive to REPs—when a broker actually runs the process.
The process: collect 12+ months of billing history and, if available, interval data from your meter. Interval data (15-minute or hourly readings) lets REPs see your actual peak profile rather than estimating it, which typically produces more competitive bids. Brief 15–25 providers simultaneously on your location (TDSP territory), typical operating hours, and any known equipment changes. Collect bids, compare all-in rates across 12-, 24-, and 36-month terms, and evaluate early termination provisions—important if practice ownership or location may change.
Timing: Start 90–120 days before contract expiration. Avoid July–August if your timeline allows—peak cooling season inflates REP hedging costs 8–12% compared to September–October renewals. For practices with near-term expirations: locking in now before summer pricing is the better outcome. For more on how Texas commercial electricity billing works, see our full guide.
Cost structure: Brokers are compensated by providers, not by the practice. Commission rates typically run $0.005–$0.010/kWh. A specialist working at the lower end ($0.003–$0.005/kWh) passes substantially more savings to the practice. Ask directly before engaging.
Reducing Demand Charges Without Compromising Patient Care
Demand management for medical practices starts with an honest acknowledgment of constraints: you cannot shift when patients arrive, how long procedures take, or sterilization cycle requirements under OSHA and state board standards. What you can manage is the sequencing of high-draw equipment within your operating window.
Autoclave and sterilizer scheduling. A standard autoclave draws 4–6 kW per cycle. Running two simultaneously during a 3 PM peak hour adds 8–12 kW to your peak demand reading. Staggering cycles—running the second sterilizer only after the first drops back to idle—reduces peak draw without changing total sterilization throughput. This is a scheduling change, not a compliance change. Typical demand reduction: 10–15%.
HVAC pre-cooling. Medical HVAC systems must maintain infection-control air exchange rates higher than standard commercial requirements (typically 4–6 air changes per hour). This makes HVAC a high-draw constant, not a flexible load. However, pre-cooling treatment and patient areas to 70°F by 1:45 PM, then allowing a 1–2°F setback during the 2–5 PM peak window, reduces compressor cycling without detectable patient discomfort. Typical demand reduction: 12–20% on HVAC load specifically.
Water heater scheduling. Tank-based water heaters for sterilization prep and hand washing can run on timers set for early morning and evening hours. Zero-cost operational change. Typical demand reduction: 5–10%.
Interval monitoring. Installing 15-minute interval monitoring ($800–$3,000) identifies exactly which equipment combination creates your monthly peak. Most practices find their peak isn’t from the equipment they expected—frequently an HVAC compressor cycling on during a simultaneous sterilization run creates the billing-period maximum. Knowing the specific trigger is the first step to managing it. ROI on monitoring: typically 18–36 months against the demand charge savings it enables.
A 5-room urgent care clinic in Houston reduced peak demand from 72 kW to 62 kW through staggered autoclave scheduling and HVAC pre-cooling alone—saving $9,200 annually on demand charges with no change to patient care or staff workflow.
Efficiency Upgrades with Measurable Payback
Medical-grade LED lighting in exam and treatment rooms. Older surgical overhead lights draw 500–1,000W each; LED retrofits run 150–300W with equivalent or superior color rendering for clinical use. Exam room LED conversion cuts lighting energy 70–75%. Waiting area and administrative lighting: 70–80% reduction. Oncor and CenterPoint rebate programs cover 30–50% of qualified LED retrofit costs. Payback after rebates: 12–18 months.
Vaccine and medication refrigerator replacement. Pre-2015 medical refrigerators consume 2–4 kWh/day continuously. Modern ENERGY STAR-qualified medical refrigerators run 25–40% more efficiently. Utility rebates: $300–$600 per unit. Payback: 18–30 months.
HVAC variable-speed air handler upgrades. If your air handling units are 12+ years old, variable-speed replacements reduce energy consumption 35–45% while maintaining required air exchange rates—this is not a compliance tradeoff. Utility rebates: $1,500–$3,000 typical. Payback: 24–48 months.
Sequencing recommendation: implement efficiency upgrades before your next contract renewal. A practice reducing monthly consumption from 22,000 kWh to 18,000 kWh before bidding gets its competitive rate applied to a smaller baseline—procurement savings and efficiency savings compound.
Two Texas Medical Practice Case Studies
Case Study 1: 2-Chair Dental Practice, Dallas (Oncor Territory)
Starting position: 14,500 kWh/month at 11.2¢/kWh = $1,624/month ($19,488/year). The practice had auto-renewed with the same provider for three consecutive years and had no interval data on file.
After competitive bid through reverse auction: 8.1¢/kWh, 24-month fixed contract. Energy charge savings: $3,360/year. Staggered autoclave scheduling and HVAC pre-cooling reduced peak demand from 38 kW to 32 kW. Demand charge savings: $1,680/year. LED retrofit of three exam rooms (Oncor rebate covered 40% of project cost): $320/year savings. Total annual savings: $5,360, a 27.5% reduction. Time from engagement to implementation: 3 weeks for procurement, 1 week for demand management setup, 5 weeks for LED retrofit completion.
Case Study 2: 4-Room Urgent Care Clinic, Houston (CenterPoint Territory)
Starting position: 28,000 kWh/month at 10.8¢/kWh = $3,024/month ($36,288/year).
After competitive bid: 7.9¢/kWh, 36-month contract. Energy charge savings: $7,840/year. HVAC pre-cooling protocol and staggered sterilization equipment scheduling reduced peak demand from 65 kW to 56 kW. Demand charge savings: $4,260/year. Two medical refrigerator replacements plus LED retrofit and smart thermostat installation: $1,200/year savings. Capital investment: $4,200. Total annual savings: $13,300, a 36.6% reduction. Payback on upgrades: under 4 months. Remaining savings: pure cash flow improvement.
Action Framework: Where to Start
Contract expires in 0–6 months: Start competitive procurement immediately— 90 days is the minimum window for real market optionality. Implement autoclave staggering and HVAC pre-cooling now; both require zero capital. Target: 22% combined savings from procurement and demand management.
Contract expires in 6–18 months: Run an efficiency audit now. Prioritize LED retrofits and medical refrigerator replacement—both qualify for utility rebates and reduce your consumption baseline before bidding. Begin procurement 4 months before expiration. Target: 28% combined savings across all three levers.
Locked in for 18+ months: Focus on demand management and efficiency upgrades now. Schedule HVAC replacement to align with your renewal window. Track ERCOT summer load forecasts each April to manage 4CP exposure. Target: 30%+ total reduction by combining all strategies at renewal.
Unsure if your current rate is fair: A bill audit requires only your last 12 months of bills and takes under 30 minutes to submit. You’ll receive a market rate comparison, identification of your demand charge exposure, and a savings projection specific to your practice type and load profile. Request a free bill analysis for your medical practice—no obligation, results within 24 hours.
Most Texas dental practices, urgent care clinics, and physician offices are leaving $8,000–$28,000 per year on the table. The path to recovery involves competitive procurement, demand management within existing operating hours, and targeted efficiency upgrades—none of which require compromising patient care, sterilization standards, or clinical operations. The only requirement is starting the process before your current contract auto-renews again.
Call (737) 295-9735 or request your free analysis online. EnergyBrokerTX, PUC License BR260054.